



Dysphagia
Definition
Dysphagia is the medical term for a swallowing disorder that can affect one or more phases of the swallowing process. In severe cases, patients may not be able to swallow at all 1.
Dysphagia can be a temporary condition (improving with rehabilitation) or a progressive and permanent disorder.
There are two main types of dysphagia:
- ropharyngeal dysphagia: Affects the mouth or throat, often due to congenital conditions (e.g., cerebral palsy) or acquired neurological disorders.
- Esophageal dysphagia: Affects the esophagus, typically due to an obstruction (e.g., esophageal cancer) or disorders of the esophageal muscles (e.g., achalasia).
Signs and Symptoms
- Pain or difficulty swallowing certain foods or fluids (odynophagia)
- Coughing or gagging during eating or drinking
- Nasal regurgitation
- Sensation of food or fluids being stuck in the throat
- Gurgling or wet-sounding voice while eating or drinking
Prevalence
The prevalence of dysphagia varies depending on the population and underlying disease:
| World Population | 8% |
| Independently Living Older Adults | 33% |
| Older Adults Living in Nursing Homes | >50% |
| Cerebrovascular Event (Stroke) | <50% |
| Traumatic Brain Injury | 60% |
| Amyotrophic Lateral Sclerosis (ALS) | >30% at Diagnosis 100% as the disease progresses |
| Multiple Sclerosis | <50% |
| Critically Ill Patients Requiring Prolonged Mechanical Ventilation | 70-80% |
Adapted from 3.
Impact on Nutritional Status
Swallowing difficulties can lead to a fear of swallowing and a reduced enjoyment of meals, which in turn contributes to reduced food and fluid intake and consequently to malnutrition and dehydration 4,5. Dysphagia also increases the risk of respiratory infections and aspiration pneumonia 3.
Loss of muscle mass (sarcopenia) due to malnutrition and dehydration also breaks down the muscles involved in swallowing. This can further impair swallowing efficiency, creating a dangerous vicious circle.
The treatment of dysphagia usually involves a multidisciplinary team, and the appropriate approach depends on the underlying cause of the condition.
Screening and Assessment Methods
- Screening Tools: The Eating Assessment Tool (EAT-10) and the Gugging Swallowing Screen (GUSS) are commonly used bedside screening tools. Diagnosis of dysphagia may involve a clinical swallowing examination and/or instrumental assessment, such as a videofluoroscopic swallowing study or a fiberoptic endoscopic swallowing study.
- Assessment by Speech or Physical Therapists: Speech therapists (or physical therapists with additional training) assess the safest consistency for solid and liquid foods using scales like the Dysphagia Outcome and Severity Scale and the Functional Oral Intake Scale.
- Prescription and Training: Based on the recommendations of speech or physical therapists, treating physicians prescribe the safest food consistency. Once a prescription is provided, dietitians train patients on handling the consistency-adapted diet and enrichment techniques. Swallowing therapists typically provide instructions on thickening fluids
Management strategies
- Consistency-adapted diet as prescribed by a doctor
- Thickening of fluids to increase viscosity
- Use of special aids and positioning/posture techniques, e.g. dysphagia cup and spoon
- Recommendation of swallowing exercises to strengthen the muscles in the mouth and throat
Oral Nutrition
Consistency-adapted foods (soft, semi-solid, or semi-liquid) and thickened fluids are often necessary to aid in compensating for a reduced oral preparation phase and to facilitate oral and pharyngeal transport.
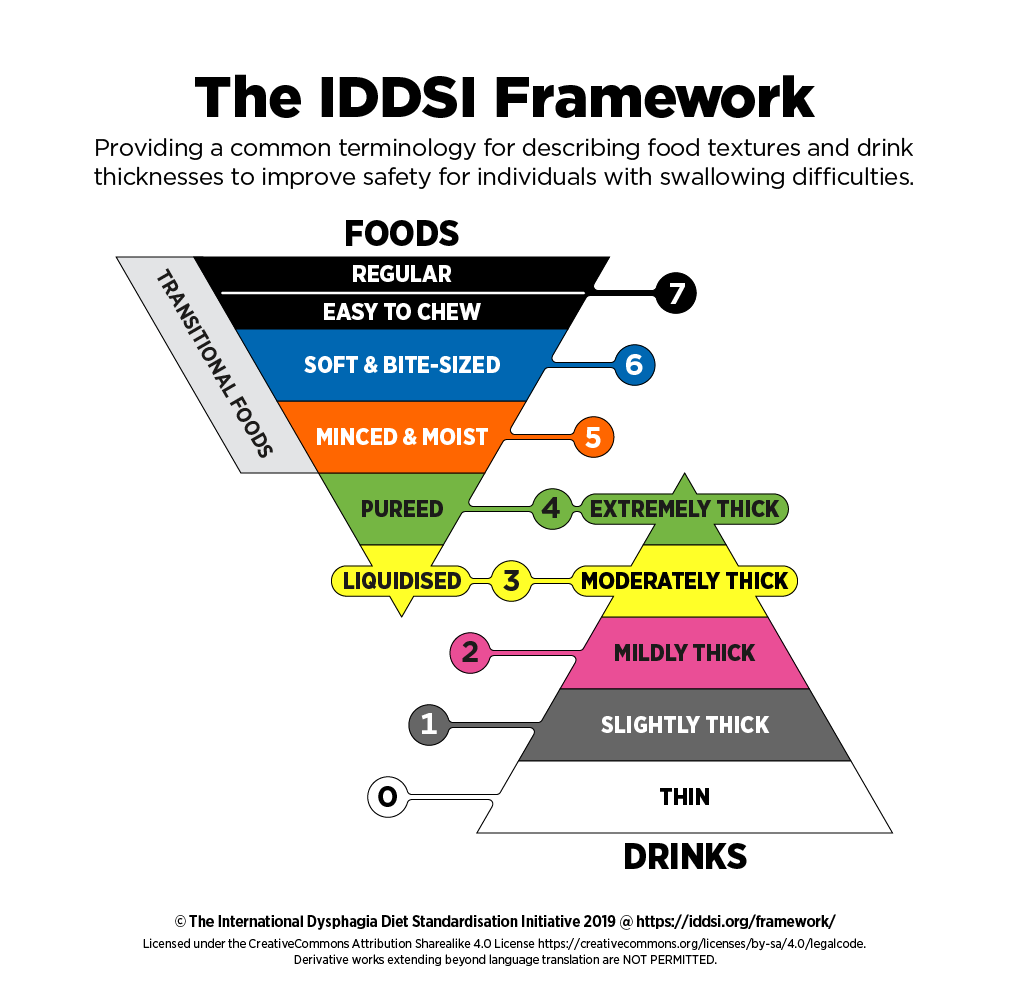
To standardize food textures and drink thickness, the International Dysphagia Diet Standardization Initiative (IDDSI) developed a common terminology in 2015. The IDDSI framework consists of 8 levels (0–7), where drinks are classified from levels 0–4, and foods from levels 3–7. Each level is assigned a number, a text label, and color codes, along with descriptions and test methods to confirm the consistency of a food or liquid 8.
The IDDSI framework has been extensively tested. The details are available on the official IDDSI website (IDDSI Terminology).
Enteral Nutrition
Oral feeding should be used whenever possible. However, in cases of severe swallowing dysfunction, enteral feeding can be used to provide adequate nutrition, hydration, and medications to patients while they regain their swallowing ability 6. Nasogastric tubes are typically used for short-term feeding (a few days to weeks), whereas gastrostomy tubes are preferred when enteral feeding is required for periods longer than four weeks. For patients who need encouragement to resume oral intake but cannot meet their nutritional needs solely through oral feeding, a combination approach can be used—providing enteral nutrition at night while allowing them to eat meals orally during the day 9.
Adequate Nutritional Value of Texture-Modified Meals
Many studies indicate that patients on a texture-modified diet consume less energy and protein compared to those on a regular diet. This may be due to the altered texture, increased difficulty in eating, and often less appealing or attractively presented foods. Additionally, the selection of foods with suitable textures can be limited. To achieve the desired consistency, liquids are frequently added, which increases meal volume while decreasing nutrient densit 10,11.
Therefore, here are some recommendations for improving consistency-adjusted nutrition 5:
- Serve several small meals throughout the day, avoiding times when the patient is particularly tired, as this can increase aspiration risk.
- Consider the patient’s preferences and dislikes to enhance acceptance.
- Enrich meals with energy- and protein-dense ingredients such as maltodextrin, protein powder, milk powder, or fats like oil and cream.
- Offer a variety of food options to reduce refusals, and present meals attractively, labeling items on the plate if necessary.
Oral Nutritional Supplements (ONS)
If food intake is insufficient, ONS are recommended 6. However, for patients with dysphagia, it is crucial to consider the level of dysphagia and ensure that ONS is provided at a safe consistency. Many manufacturers offer pre-thickened ONS to align with different IDDSI levels and produce thickening agents (e.g., starch-based or gum-based) that can be added as needed.
Fluid Intake
While thickened fluids are necessary to achieve a safe consistency for people with dysphagia, they significantly reduce overall fluid intake 12. Recommendations to minimize this effect include:
- Adding the minimum amount of thickening agent required to achieve safety.
- Enhancing palatability by using flavored thickening agents or adding simple thickeners to flavored water or juices.
- Use of pre-thickened and flavored water, which is more convenient and better accepted but typically more expensive. For selected patients, discussing the potential use of the Frazier/Free Water protocol with the multidisciplinary team to allow unthickened water between meals as appropriate, balancing safety with practicality.
Micronutrient Needs
Due to limited food intake and variety, many patients may have deficiencies in vitamins and minerals. It is essential to assess and monitor these potential deficiencies and consider micronutrient supplementation at an appropriate consistency to meet individual needs 2.
When administering medication to patients with dysphagia, it is essential to reduce the amount or frequency of oral medication when appropriate and to discontinue any unnecessary medications 13.
Patients with dysphagia may be unable to swallow tablets or capsules safely. Therefore, liquid medications are the preferred method of administration but should only be used if they are thickened to the appropriate consistency for safe swallowing 13.
For further information, consult the hospital pharmacy and the NEWT guidelines. The table below provides information on administering medications to people with dysphagia or those with feeding tubes 14.
Interactions between medications and food (for example, certain medications should not be taken with milk) and interactions between medications and thickening agents (for instance, there is a known interaction between macrogol laxatives and starch-based thickening agents) should also be taken into consideration 13.
Type of Formulation |
Indication |
| Standard Tablets | Can generally be administered normally. Crushing tablets is almost always outside the scope of approval (product license). If tablets need to be halved, tablet splitters should be used. |
| Coated Tablets (Dragees) and Film-Coated Tablets | Generally suitable for crushing. |
| Enteric-Coated Tablets | Do not crush. This type of formulation should not be used in a crushed form, as unwanted side effects may occur. |
|
Buccal and Sublingual Tablets |
Do not crush. Can generally be administered normally if the patient can hold the tablets safely in the mouth. |
| Chewable Tablets | Do not crush. Can generally be administered in the usual way. |
| Modified and Controlled Release Formulations | Do not crush. Switching to a formulation with immediate-release is necessary. Some modified-release formulations can be administered whole with an appropriate food consistency. |
| Cytotoxic Medications | Avoid contact. Do not crush. |
| Capsules | Opening capsules is almost always outside the scope of approval (product license). If this is the case, then do not use this type of formulation. |
| Dispersible and Effervescent Tablets | Can generally be administered in the usual way by mixing with water and adjusting to the appropriate consistency if indicated (unless specifically stated otherwise in the product information). |
Adapted from NEWT guidelines 14
- Malagelada JR, Bazzoli F, Boeckxstaens G, De Looze D, Fried M, Kahrilas P, et al. World gastroenterology organisation global guidelines: dysphagia--global guidelines and cascades update September 2014. J Clin Gastroenterol. 2015;49(5):370-8.
- FAND JLRMRCaKMMR. Krause and Mahan's Food & the Nutrition Care Process. 15th Edition ed2020.
- Burgos R, Bretón I, Cereda E, Desport JC, Dziewas R, Genton L, et al. ESPEN guideline clinical nutrition in neurology. Clin Nutr. 2018;37(1):354-96.
- Volkert D, Beck AM, Cederholm T, Cruz-Jentoft A, Goisser S, Hooper L, et al. ESPEN guideline on clinical nutrition and hydration in geriatrics. Clin Nutr. 2019;38(1):10-47.
- Ballesteros-Pomar MD, Cherubini A, Keller H, Lam P, Rolland Y, Simmons SF. Texture-Modified Diet for Improving the Management of Oropharyngeal Dysphagia in Nursing Home Residents: An Expert Review. J Nutr Health Aging. 2020;24(6):576-81.
- Wirth R, Dziewas R, Beck AM, Clavé P, Hamdy S, Heppner HJ, et al. Oropharyngeal dysphagia in older persons - from pathophysiology to adequate intervention: a review and summary of an international expert meeting. Clin Interv Aging. 2016;11:189-208.
- Doan T-N, Ho W-C, Wang L-H, Chang F-C, Nhu NT, Chou L-W. Prevalence and Methods for Assessment of Oropharyngeal Dysphagia in Older Adults: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2022;11(9):2605.
- Cichero JA, Lam P, Steele CM, Hanson B, Chen J, Dantas RO, et al. Development of International Terminology and Definitions for Texture-Modified Foods and Thickened Fluids Used in Dysphagia Management: The IDDSI Framework. Dysphagia. 2017;32(2):293-314.
- Bischoff SC, Austin P, Boeykens K, Chourdakis M, Cuerda C, Jonkers-Schuitema C, et al. ESPEN practical guideline: Home enteral nutrition. Clin Nutr. 2022;41(2):468-88.
- Wright L, Cotter D, Hickson M, Frost G. Comparison of energy and protein intakes of older people consuming a texture modified diet with a normal hospital diet. J Hum Nutr Diet. 2005;18(3):213-9.
- Sura L, Madhavan A, Carnaby G, Crary MA. Dysphagia in the elderly: management and nutritional considerations. Clin Interv Aging. 2012;7:287-98.
- Cichero JA. Thickening agents used for dysphagia management: effect on bioavailability of water, medication and feelings of satiety. Nutr J. 2013;12:54.
- Service UKNH. Choosing formulations of medicines for adults with swallowing difficulties June 2021 [
- Department WMH-P. The NEWT Guidelines for administration of medication to patients with enteral feeding tubes or swallowing difficulties2006.
Authorship:
Ines Moreira, MD, NOVA Medical School, Universidade NOVA de Lisboa
Joana Ferreira, MD, NOVA Medical School, Universidade NOVA de Lisboa

{kind=link}